To this debate between Jonah Goldberg and Henry Farrell, about whether culture is properly considered when evaluating the merits of European welfare states, I'm compelled to introduce a piece of evidence. (Let me catch you up: Goldberg says that France's healthcare system is too teat-suckingly Frrrrrrránch to work on Americans, what with their Protestant ethic and tradition of self reliance. Farrell says this is stupid: a deeply unserious encomium to fixed national values, which are subject to disagreement and rapid change and, in any case, shouldn't be the markers of our destiny. Goldberg clarifies that he alone among the left and right is assigning culture the non-zero significance it should hold in health care policy decisions. Farrell says this is stoopid: a "two-step of terrific triviality".)
Below the cut, then, is an (arguably NSFW) ad from France that someone e-mailed to me:

As far as I can tell, it's legit—a print ad campaign by Aides (a French nonprofit, founded by Daniel Defert after Michel Foucault's death, that promotes awareness and good health). If at all possible, I'd rather not pay tax dollars toward these.
Okay, fine, so this campaign is neither here nor there w/r/t the blogospheric health care debate. But it does really drive home the values divide between colonies and continent when it comes to health, and in particular sexual health.
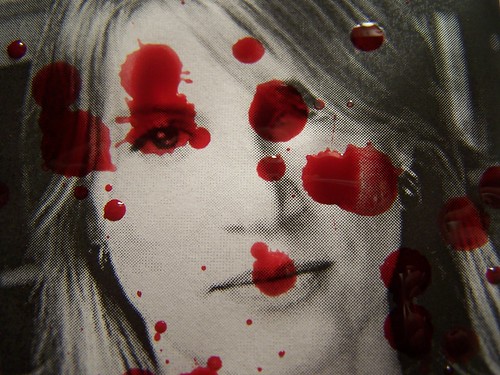
Assuming it's legit, it's something that, I imagine, wouldn't pass without comment even in gay old Europe. Tres risqué. But not even were real-life, person-sized, sex-hungry insectoids prowling ur MySpaces would you find this warning posted on a Big State campus kiosk. It's not the squicky image that makes the campaign so outrageous—well, not that entirely, or rather not the first-order squickiness of the image.
Bathing the character of good health in white (white skin, white linens, white furniture: white light, white heat)—while painting the sexual predator as darkest ebony—plays on a well-worn, white=good, black=evilbadevil metaphor system. Notwithstanding 300, Katrina news coverage, Imus in the morning, etc., this is a visual that doesn't play in America. At least, not without criticism. Especially when the topic is AIDS, it shouldn't have any purchase: In the States, nearly half of all HIV-infected people are black, 2 percent of African Americans have HIV—the horrifying statistics go on. Phil Wilson, founder of the Black AIDS Institute, says correctly, "AIDS is a black disease, full stock, through all lenses."
In France, however, integration is an enormous social problem, and this ad speaks to a characteristic myopia that traditionalists have on the subject of race. It also reveals a society that's perhaps unclear about HIV/AIDS squares with people. (Not to mention how the virus is transmitted.) Perhaps the less-alarming incidence rates in France makes for a disease that is ultimately more frightening—hence, monsters run amok with a venomous, sexually transmitted disease, rather than people living with a chronic, sexually transmitted infection.
The good things you can say about the ad, however, are the things disqualify it from the American public square. Kudos to the French for showing both a man and a woman enjoying sex. These look like hetero pairings, but hey, I'm no entomologist—there's room for straight and gay alike to be squicked out. However they're doing it, one thing's certain: These people are enjoying sex. Say what you will about arachnids, but spider is clearly getting the job done. And our totally hott monsieur appears to be enjoying some GGG, dangerous, kinky action. Also: man butt! This ad's right out. Stateside, sex and AIDS are fairly graphically divorced. A stars-and-stripes AIDS campaign would encourage you to abstain from fucking bugs until you're married.
Is there a trans-Atlantic message to take away: a message that bridges cultures? Don't fuck bugs? Kids et gosses: Ne baisez pas les bogues. Au moins, pas sans préservatif.















 BACKGROUND: Providing HIV treatment in less developed countries is a global priority. Most programs focus exclusively on antiretroviral therapy (ART) and on patients with advanced HIV disease. In contrast, the MTCT-Plus Initiative has established comprehensive family-centered HIV programs in less developed countries.
BACKGROUND: Providing HIV treatment in less developed countries is a global priority. Most programs focus exclusively on antiretroviral therapy (ART) and on patients with advanced HIV disease. In contrast, the MTCT-Plus Initiative has established comprehensive family-centered HIV programs in less developed countries. The researchers cited a biological reason that might explain the findings. They said the mucous membrane within the intestines may serve as a barrier to HIV infection, and that breast milk could reinforce and protect that lining.
The researchers cited a biological reason that might explain the findings. They said the mucous membrane within the intestines may serve as a barrier to HIV infection, and that breast milk could reinforce and protect that lining.






 13 years) living with AIDS between 1999 and 2004 who were reported to the New York City HIV/AIDS Reporting System and Vital Statistics Registry through 2004 (n = 68 669).
13 years) living with AIDS between 1999 and 2004 who were reported to the New York City HIV/AIDS Reporting System and Vital Statistics Registry through 2004 (n = 68 669). 








{kind=link}
{kind=link}
{kind=link}